
This article assesses the quality and outcomes of research into forms of complementary and alternative medicine: intercessory prayer, therapeutic touch, Reiki, Johrei and other forms of spiritual or distant healing. The existing research is found to be suggestive of significant effects, although a lack of rigour across most studies means no positive conclusions can as yet be drawn with confidence.
Contents
Intercessory Prayer
Intercessory prayer (IP) is defined as the act of petitioning a higher power on behalf of someone else.1Dossey (1993). In a 2002 survey of American adults, the Centers for Disease Control and Prevention found that 62% had used complementary and alternative medicine – that is, methods of treatment that fall outside the realm of conventional (or allopathic) medicine – in the last twelve months. Of those 62%, 24.4% used IP, making this the second most popular form of complementary and alternative medicine after prayer for one’s own health. Prayer is a part of almost every major religion in the world;2Andrade & Radhakrishnan (2009); Benor (2001); Masters (2005); Masters, Spielmans, & Goodson (2006); Roberts, Ahmed, Hall, & Davison (2009). how one prays, and to whom or what, depends not only on one’s religious or spiritual orientation but also on one’s personal preference.
The scientific investigation of IP raises issues that are not present in the investigation of other forms of spiritual healing. Each will be discussed individually.
Directed or Non-Directed Prayer?
The idiosyncratic nature of prayer is the root of one issue of research specific to IP: whether intercessors should use directed or non-directed prayer. Directed prayers are prayers in which intercessors ask their Higher Power to make manifest specific objectives. Non-directed prayers are prayers which ask for the will of a Higher Power to be made manifest (whatever that will may be), or that ask for whatever is best for the intercessee, such as ‘Thy will be done’.3Dossey (1993).
There are strengths and weaknesses to both approaches. Directed prayer appears the most sensible approach to take from a research perspective: telling intercessors what to pray for means that researchers can ensure they are petitioning for health and well-being changes that are being measured. Directed prayer also improves the validity of research, ensuring that all intercessors are providing the same ‘treatment’ and allowing for other researchers to replicate one’s methodology more completely.
However, prayer is a very personal activity, and to homogenize it for the sake of research may be counterproductive. Directing intercessors how to pray may result in inauthentic prayers, as people may not feel the same connection with the divine that they feel when praying normally. Not only could this reduce the ecological validity of the study (as intercessors may not be praying in their usual fashion), it could also influence the efficacy of the practice: intercessors may not feel comfortable with the style of prayer prescribed to them, or may be distracted by conducting a familiar activity in a new way, possibly resulting in reduced concentration or absorption in prayer.
Some intercessors may feel more comfortable with the non-directed approach, as it could be considered presumptuous for a person to dictate to a Higher Power what form an intervention should take. One drawback to this approach is that when prayer is non-directed one is even less certain how the intervention will manifest, leaving open the possibility that it will present by unmeasured means, resulting in a type II error (false negative). Another possible shortcoming of this approach is that what is best for the individual is not always survival, for example a person suffering from an agonizing terminal condition. Both approaches are valid ways of measuring IP, and both have produced significant research results.4Dossey (1993).
Impure Control Groups
The prevalence of IP causes difficulties in research, especially within those studies that utilize clinical samples: participants who are ill are extremely likely to have friends or family members praying for them, and even if they do not, many people say intercessory prayers for people around the world who are sick or suffering.5Masters, Spielmans, & Goodson (2006); Roberts, Ahmed, Hall, & Davison (2009); Cohen et al. (2000) This means that even those who are in the control group (the group that does not receive the intervention and to which the intervention group is compared) are likely to be in receipt of IP, resulting in a ‘contaminated’ control group resulting in the true effect of IP being masked. However, it likewise means that participants in the active conditions (those receiving IP) are also possibly receiving IP from friends and family members. This would mean there is likely to be a background level of prayer evenly distributed between the two groups,6Cohen et al. (2000). suggesting that the issue of contamination is not necessarily important.
The Involvement of Deity
One question is whether the effectiveness of healing interventions can be determined through outcome measures, a universal issue in research into spiritual healing, but more complex in the case of IP, given the potential involvement of a divine power. Some argue that, as prayer is more than merely a way of placing an order with God (it is also a way to commune with the divine), so apparent non-fulfilment of requests made in prayers (as evidenced by non-significant changes in outcome measures) does not necessarily equate to inefficacy of prayer, as those same prayers may have helped the person praying to feel closer to the divine.7Cohen et al. (2000); Jonas & Linde (2002). These arguments make sense when discussing regular personal prayer, but can the same be said for intercessory prayer, the point of which is to request an intervention on behalf of someone else?
It has been suggested that spiritual healing should not be investigated scientifically in the absence of a plausible explanation of the underlying mechanism.8Masters, Spielmans, & Goodson (2006); O’Mathúna et al. (2002). This issue is yet more complex within IP research, given the addition of deity: is the effect caused by the actions of those praying, or rather by the intervention of the divine being to whom the petitions are addressed? Most researchers prefer the former, as reflected in the following comments:
Our study focused only on intercessory prayer as provided in this trial, and was never intended to, and cannot, address a large number of religious questions, such as whether God exists, whether God answers intercessory prayers, or whether prayers from one religious group work in the same way as prayers from other groups.9Benson et al. (2006).
… we have not proven that God answers prayers or that God even exists. It was intercessory prayer, not the existence of God, that was tested here.10Harris et al. (1999).
IP trials are not designed to determine whether God exists, whether God does or does not respond to IP… or to put God to the test. IP trials focus only on the effects of additional IP on outcomes after a medical procedure or illness…11Jonas & Linde (2002).
These quotes demonstrate that the primary concern of many investigators is to first establish whether or not an effect exists, rather than to try to prove the mechanism. It is possible to test to see if an intervention has an effect, and, once its efficacy has been established, to then investigate the means by which it works – as is common within general medicine, for example aspirin, digitalis, radiotherapy and oophorectomies.12Halperin (2001).
Not everyone agrees that investigating IP need not mean testing the existence of a divine power. Some feel that that to study IP is, by default, to test God and therefore offensive to religion.13Halperin (2001). Paul argues that if petitions made to a deity on behalf of another person, without that person’s knowledge, are proven to be successful, then many would justifiably interpret those results as evidence of the existence of a higher power.14Paul (2008). Andrade and Radhakrishnan agree, stating that, as IP studies usually involve intercessors having no contact with – and very little identifying information about – the intercessees, it is up to the omniscient deity being petitioned to intercede for the correct target.15Andrade & Radhakrishnan (2009). Pande too concurs, stating in response to the paper by Harris et al.:16Harris et al.(1999). ‘If the intent of the study was to determine whether God answers prayer, then God’s will and His existence were also being tested de facto, since the prayer was directed to God for the healing of 466 patients in the prayer group.’17Pande (2000). Harris et al. would likely argue that they were not attempting to determine if God answers prayer, only the effect which is elicited as a result of intercessory prayer, which may or may not be the actions of God: ‘…It was intercessory prayer, not the existence of God, that was tested here.’18Harris et al. (1999). Masters asks, if it was not the intention of Harris et al. to test whether or not God answers prayers, why then did they specify that intercessors had to believe in a personal God who responds to intercessory prayer?19Masters (2005). In answer, Walach argues that the most important influence on the efficacy of any type of healing is the belief of the therapist/healer that their mode of healing is effective, it being of no consequence whether or not this belief is correct.20Walach (2007). Benor and Levin also support the theory that it is the healer that is the most important aspect of healing, and not the methods utilized.21Benor (2001); Levin (2011). This suggests that it is entirely possible to study IP without the intention to test God, whilst still requiring true believers to participate as intercessors.
Summary
Prayer is one of the most common ways to attempt healing and yet one of the most difficult to study empirically. Being personal and idiosyncratic, the action of prayer is difficult to standardize without affecting ecological validity. Also, because prayer ascribes to the concept of a sentient supreme being, questions of mechanism (whilst possibly premature) involve not only physics but also theology.
Evidence
Despite the difficulties, much IP research has been carried out, prompting a succession of reviews and meta-analyses. This enables an overview to be given of the current state of research, with assessments not only of the results achieved so far but also an appraisal of the quality of the research.
Reviews and Meta-Analyses
Powell, Shahabi and Thoresen conducted a review of research investigating the impact of various religious and spiritual practices on physical health, to evaluate the plausibility of theories about the connection between the two. To be included in the review, studies had to conform to stringent methodological criteria, to ensure that only the most valid evidence was used. Studies had to adequately control for confounding demographic and health variables, to ensure that any effect found was the result of the behaviour or practice investigated and not an artefact.
Only three studies investigating the efficacy of IP conformed to the criteria for inclusion. All of these studies provided mixed evidence for the efficacy of IP, with the majority of significant effects being seen in subjective measures of health, rather than the physical measures. All of the studies in the review were given a quality rating of ‘B’, meaning that they were generally methodologically sound but had at least one flaw that could have influenced the results, such as inadequate control for confounds, or failure to control for multiple tests. Powell, Shahabi and Thoresen conclude that ‘there is some evidence to support the hypothesis that being prayed for improves recovery from acute illness’, and emphasize the importance of well controlled, flaw-free study designs in future research.22Powell, Shahabi & Thoresen (2003).
Hodge conducted a meta-analysis of empirical research into IP. Meta-analysis is the drawing together of research on one specific topic and subjecting it to analysis to give an overall effect size. A social work database, a psychology database and a medical research database were searched, resulting in seventeen studies that conformed to the inclusion criteria. Hodge analysed the omnibus effect size using both a random effects and a fixed effects model, as he believes that both are appropriate for this research.23Hodge, (2007). The fixed effects model works on the assumption that ‘…there is one true effect size…which underlies all the studies in the analysis and that all differences in observed effects are due to sampling error.’ Conversely, the random effects model assumes ‘…that the true effect could vary from study to study … because the studies will differ in mixes of participants and in the implementations of intervention …’24Borenstein, Hedges, Higgins, & Rothstein (2009).
Both models showed a small significant effect for intercessory prayer (random effect: g= -.171, p = .015, fixed effects g = -.095, p = .006). The analyses were also conducted without the inclusion of a paper by Cha, Wirth & Lobo,25Cha, Wirth, & Lobo (2001). the legitimacy of which has been questioned.26Harris et al. (1999); Flamm (2004, October). Once this study had been removed, only the more conservative fixed effects model showed a significant, small effect (g= -.077, p =.031), while the random effects model was non-significant (g= -.109, p =.062). Hodge acknowledges that ‘the synthesis of outcomes across studies produced small, but significant, effects for intercessory prayer’, but concedes that, given the many issues around successfully applying IP as an intervention, some may not consider the results sufficiently convincing to justify using IP as a clinical intervention.27Hodge, (2007).
Roberts, Ahmed, Hall and Davison6 conducted a review of randomized trials investigating the efficacy of IP for the Cochrane collaboration. They searched a number of medical and religious research databases and found ten papers eligible for review, the criteria being that they included both an IP and routine care group and used the RCT design. The studies they reviewed had a combined n of 7,807; participants in the studies had a range of health issues; prayers were conducted by intercessors from a variety of faiths and denominations; and efficacy was assessed using a number of different measures. Thirty-three various possible complications were included across the studies as possible outcomes, of which only three showed any significant influence of IP. Fewer participants receiving IP suffered cardiac arrest (three studies, n = 2174, RR = .46, CI 0.21-0.99) fewer participants required catheterization (one study, n =990, RR 0.80, CI 0.66-0.98) and fewer participants required major surgery (two studies, n = 1383, RR 0.69, CI 0.51-0.95). There were no significant differences between groups on the other outcome measures of mortality (six studies, n =6784, RR.077, CI 0.51-1.16), clinical state (five studies, n = 2705, RR 0.98, CI 0.86-1.11), change in attitude (one study, n= 38. RR 0.94 CI 0.73-1.21), readmission to hospital (two studies, n = 1155. RR 0.93 CI .071-1.22), admission to A & E (one study, n =1789, RR 1.28, CI 0.73-2.24) or leaving the study early (eight studies, n = 7.38, RR 0.75 CI 0.43-1.31). Length of stay in hospital and length of stay in CCU (coronary care unit) were found to be equivocal, and statistics are not given.28Roberts, Ahmed, Hall, & Davison (2009).
While these findings may appear bleak for proponents of IP, Roberts et al. do not discount the possibility of an effect of IP. They point out that certain aspects of the methodologies of the studies included in the review such as blinding (hiding which group the participants are in, whether the intervention or control group), concealment (how well the information was hidden) and randomization processes were not well described and that these weaknesses are sufficient to disguise a tangible benefit effect. Roberts et al. conclude that ‘the evidence presented so far is interesting enough to support further study’, although they recommend that IP research should not be given priority over other types of treatment research.29Roberts, Ahmed, Hall, & Davison (2009).
Masters, Spielmans & Goodson conducted a meta-analysis of fourteen studies investigating the effect of distant intercessory prayer using human participants. They found no significant effect for intercessory prayer overall (g = .100); however, when using participant health as a moderator variable, they found a small significant effect in studies that used a sick population (g = .169), but still no effect for studies using a healthy population (g = -.061). Unfortunately, this result was largely influenced by the inclusion of a paper conducted by Wirth, whose work has been rendered suspect as a result of a number of fraud charges and concerns regarding the methodology of the study in question.30Flamm (2004, October). When this study was removed, Masters et al. found no significant effect for intercessory prayer in studies using a sick population (g = .066), while the results for studies using healthy populations remained unchanged.31Masters, Spielmans, & Goodson (2006).
Astin, Harkness and Ernst conducted a systematic review of empirical studies of many forms of spiritual healing, which they separated into three groups for analysis: therapeutic touch (which will be discussed later in this chapter), prayer and other distant healing. To be included, studies had to conform to strict criteria, the aim of which was to ensure that only the highest quality studies were included in the review. Effect sizes were measured for each of the three groups, despite the researchers not taking a meta-analysis approach due to heterogeneity of the studies. Both medical and psychological research databases were searched, resulting in five studies of IP eligible for review. The combined effect size was d =0.25 (p =0.009) which is considered to be small but significant.32Astin, Harkness, & Ernst, E. (2000).
Although this finding supports the efficacy of IP, Astin et al. point out that a number of the studies in the review (not just those in the IP group) showed methodological limitations, including insufficient statistical power, heterogeneous patient groups, inadequate control of baseline measures, and insufficient blinding. These limitations, however, were not significantly correlated with effect size (R = -.15, p = >.02), suggesting that the positive results were not the result of artefacts.
Astin et al. conclude that their findings ‘… are in basic agreement with a recent Cochrane collaboration systematic review…and found no clear evidence for or against the incorporation of prayer into medical practice’, and call for further, more rigorous research.33Astin, Harkness, & Ernst, E. (2000).
Roe, Sonnex & Roxburgh likewise conducted a meta-analysis of a multitude of different approaches to spiritual healing, and grouped results by the healing approach used. Eleven studies of intercessory prayer conformed to their inclusion criteria, giving a small effect size (r=0.173). However, the results were very heterogeneous and five outliers had to be removed to render the results homogenous.Although the effect size reduced, it was still present (r= 0.138). Roe et al. found that the study quality across all of the approaches was fairly low; that the correlation between effect size and randomization method was significant; and that the correlations were suggestive between effect size and control of extraneous variables, average quality rating and clear specification of planned analysis.However, even after controlling for these aspects of methodological quality, a small effect size (for all types of non-contact healing approaches) remained (r= 0.115).34Roe, Sonnex, & Roxburgh (2015).
Table 1 shows a summary of the reviews and meta-analyses:
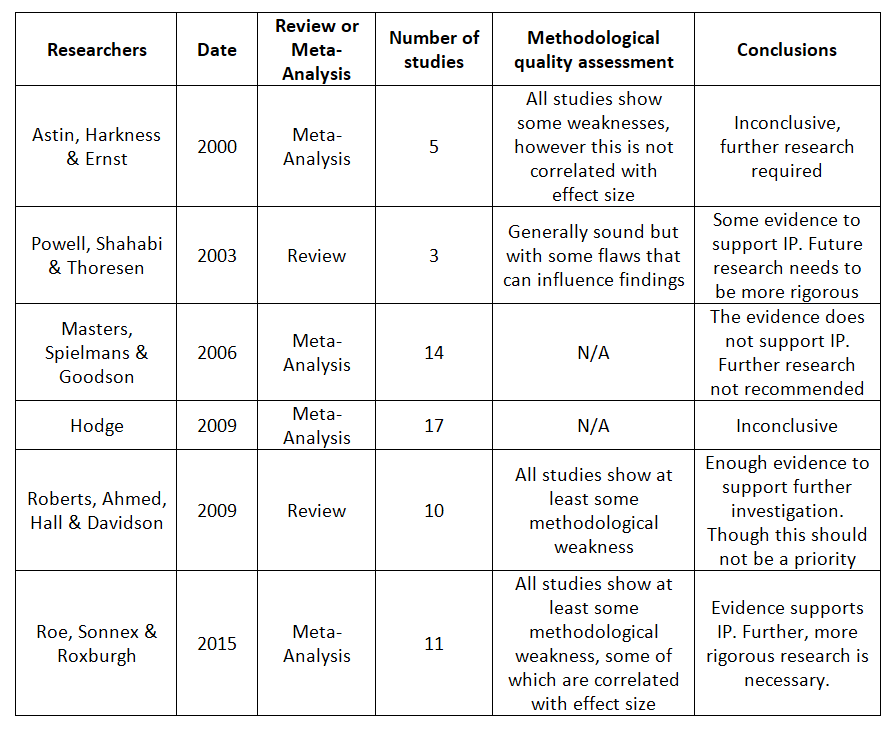
The findings of these reviews are somewhat inconclusive: whilst half the reviews do show some effect of IP, many of the issues around study design as mentioned by Roberts et al., Astin et al., and Roe, Sonnex and Roxburgh35Roberts, Ahmed, Hall, & Davison (2009); Astin, Harkness & Ernst (2000); Roe, Sonnex & Roxburgh (2015). somewhat temper the strength of this evidence. However, both Astin et al. and Roe, Sonnex and Roxburgh conclude that effects are still present even after controlling for poor quality studies, suggesting that the effect seen cannot be fully explained by weak study design.
Example of Strong Methodology
Given that the research supports further study in this area,36Roberts, Ahmed, Hall, & Davison (2009); Powell, Shahabi, & Thoresen (2003); Astin, Harkness & Ernst (2000); Roe, Sonnex & Roxburgh (2015). it is important that future researchers design studies of IP in such a way as to avoid the methodological weaknesses that diminish the impact of any significant results they may find.
One example of a methodologically sound study of IP is that by Byrd. Three hundred and ninety-three coronary-care unit patients were randomly assigned on a double blind basis to either a control or a prayer group. Each participant in the prayer group was assigned to between three and seven intercessors. Intercessors were given the patient’s name, diagnosis, general condition and updates of their condition throughout the trial. The intercessors themselves were from a variety of protestant and Roman Catholic churches, the only conditions to becoming an intercessor being that they had to be ‘born again’ according to the Gospel of John 3:3 and that they ‘…lead an active Christian life as manifested by daily devotional prayer and active Christian fellowship with a local church.’ Intercessory prayer was conducted daily, outside of the hospital, however no duration was reported. The prayers asked for a ‘… rapid recovery and for preventions of complications and death, in addition to other areas of prayer they believed to be beneficial to the patient.’ The prayer group had significantly fewer cases of pneumonia (p =<.03), congestive heart failure (p =<.03), intubation/ventilation (p =<.002), cardio pulmonary arrest (p =<.02) and significantly less need for antibiotics (p =<.005) and diuretics (p = <.05). Significantly more participants in the prayer group also showed a ‘good’ hospital course (p =<.01), that is, ‘ … no new diagnoses problems or therapies were recorded for the patient or if events occurred that only minimally increased the patient’s morbidity or risk of death.’37Byrd (1988).
Benor carried out an extensive review of spiritual healing studies, which he rated for methodological quality. Benor gave the Byrd study the highest rating for methodological quality, meaning that the study included ‘…all the items required for a blinded randomized controlled study, with adequate reporting of the data to confirm the results … This is an excellent study … it was well designed … and produced positive results with distant healing in patients with severe cardiac problems.’38Benor (2001).
This study is considered to be methodologically sound for a number of reasons. The random allocation was done using a computer generated list rather than by other methods, which may be susceptible to influences such as coin tosses or die rolls, or methods that are not truly random, such as alternate allocation or allocation by date of birth. The study used a triple blind design in which participants, researchers and hospital staff were unaware of participants’ group allocation: the use of such strong blinding helps to eliminate the possibility of bias or placebo effect. Finally, the study had a large number of participants, meaning that statistical power is not an issue.
Summary
The research that has been carried out in this field has been of varying quality and has produced varying results, but is nonetheless suggestive of some effect of IP, thus justifying further research whilst also exemplifying the importance of rigorous study design in this area. Future research needs to address the shortcomings identified in the reviews and meta-analyses discussed, by using random allocation or to sufficiently control for influencing factors such as demographics. Adequate blinding and concealment are also important, as is ensuring adequate statistical power.
Therapeutic Touch
Therapeutic Touch (TT) can be understood as a standardized version of ‘laying on of hands’, an ancient healing practice which involves healers placing their hands on or above the patient with the express intent of bringing about healing.39Benor (2001); Kreiger (1975). The practice was developed by Dolores Krieger, a professor of nursing at New York University, and Dora Kunz, a healer and clairsentient, in 1972.40Benor (2001); Levin (2011); Pumpkin Hollow Farm (2004). Krieger defines the process as ‘ … the simple placing of the hands for about 10-15 minutes on or close to the body of an ill person by someone who intends to help or heal that person.’41Kreiger (1975). Krieger states that the intention to heal is critical. Whilst she acknowledges that the concept of healing by laying on of hands is both ancient and universal, Krieger understands the mechanism behind TT from a Hindu perspective, stating that TT works through an exchange of prana, a Sanskrit word which can loosely be translated as vigour or vitality. A healthy person has a profusion of prana, whereas an ill person has a shortage; in TT Prana is transferred at will from one person to another to help address any deficits.
This process of energy exchange involves five steps:
- Centring: becoming still and reaching for a focused state.
- Assessment: moving hands over the body to identify imbalances or obstructions in the energy field.
- Unruffling: moving hands to facilitate the free flow of energy through the body (this is generally done with the hands above the body but can also involve direct physical contact).42O’Mathúna et al. (2002).
- Directing and modulating energy: energy is directed to areas of the body that are detected to be blocked or congested in order to restore balance.
- Stopping: when energy balance has been restored.
TT and Allopathic Medicine
TT has many strengths from both a research and practice perspective, by virtue of its strong links with allopathic (conventional) medicine. The majority of TT practitioners are those with a foundation in allopathic medicine (such as doctors and nurses) and the fact that Krieger herself is a nursing professor is evidenced in the symptom-oriented approach: TT involves the assessment phase, which aims to identify the client’s specific issues or illness. This, combined with its grounding in research, means it can be taught to medical practitioners without too much of a challenge to their current medical understandings.43Benor (2001). Despite being symptom oriented, TT is still a holistic approach, as it emphasizes the importance of the practitioners themselves being centred and in good health.44Levin (2011). TT’s structured method allows for standardized training and certification, which has benefits for both consumers and researchers. Consumers can be reassured that certified practitioners are knowledgeable and experienced, and researchers can be confident of replicability of TT experiments.
The limitations of this approach are few, but like the benefits are related to TT’s grounding in allopathic medicine. Benor points out that there is a risk of practitioners becoming too focused on physical symptoms and neglecting the more holistic aspects of healing, such as emotional or spiritual health, or aiding recipients to ‘find their highest potential’.45Benor (2001). Research has provided strong evidence for the efficacy of TT, which however can also lead to some practitioners becoming discriminatory of other, less well-evidenced forms of healing and thus lose sight of the fact that TT is still considered to be a form of spiritual healing.
TT appears to successfully balance both the allopathic and holistic approaches to medicine. The element of ‘diagnosis’ involved in the assessment stage dictates, to some extent, the ‘treatment’ stage of directing and modulating energy, allowing conventional medical practitioners to relate to an approach they might otherwise consider counter to their training and understanding of health and medicine. That TT works with ‘energy’, and emphasizes the importance of an all-encompassing approach to health, is an indicator of its holistic foundations. The disadvantages of this approach are not directly related to the method of healing itself, but rather are related to the practitioners: being mostly conventional medical professionals, they may neglect holistic aspects and become dismissive of other spiritual healing methods.
Evidence
There is a large body of research into the efficacy of TT. This has resulted in reviews and meta-analyses, providing a broad view of the results found so far and an evaluation of methodological quality.
Reviews and Meta-Analyses
Peters conducted a meta-analysis of therapeutic touch studies published between 1986 and 1996, searching a nursing database, a biomedical database and a psychology database. Criteria for inclusion were that the studies were empirical research that used human participants; that the TT intervention followed the phases developed by Krieger (described in detail in the above section); and that the study design included a comparison group that had not received the intervention. Nine studies found were eligible for inclusion; studies were also subject to quality assessment using the ‘quality of study’ instrument. The studies ranged in quality from a low 1.27 to a medium 2.70 with an average of 2.13.46Peters (1999).
Peters separated the analysis into ‘between group’ effects (comparing the intervention group to a control group) and ‘within group’ effects (looking at changes in one group from prior to healing being administered to after healing being administered) for psychological and physiological outcomes, in an effort to analyse homogenous outcomes. The effect size for the physiological ‘between group’ measures was d =1.20, which is a large effect. This effect size was largely influenced by two studies of poor methodological quality. Once they had been removed the effect size reduced to a medium d =.61. The effect size for ‘within groups’ physiological measures could only be calculated using two studies, though they were both of high methodological quality: the effect size was a large d =1.22. The ‘within group’ psychological measures showed a medium effect size of d =.72, once a low quality outlier had been removed. The ‘between group’ psychological measures showed a medium effect size of d =.48.
Overall, the meta-analysis provides evidence to support the efficacy of TT as a healing intervention: even with methodologically weak studies removed, a medium effect size is seen across all outcomes and designs. That the removal of weak studies resulted in a decrease in effect size however, suggests that the effects seen are not purely the result of the TT interventions, but could be the results of artefacts created by poor study design. Poor blinding or concealment, for example, can result in participants or researchers discovering group allocation which in turn can result in expectancy or placebo effects.
Peters states that further research into TT needs to address four main weaknesses: randomization procedures, intervention practice, practitioner skill and under-reporting of data. However, all of these weaknesses are the result of insufficient information within the study reports. As most of the studies in the review used convenience sampling (recruiting any available participants regardless of demographics, health status, etc.), Peters stresses the importance of random group assignment (assigning participants to either the control or intervention group randomly to ensure groups are evenly matched). But he also points out that, within the majority of study reports, assignment practices were not clearly outlined, thus raising questions about the results. The under-reporting of data, specifically, presents in two ways: of demographic information and of statistics for non-significant findings. Under-reporting of demographics means that the impact of these factors cannot be established, and therefore controlled for, to get an image of the true effect. The under-reporting of statistics for non-significant findings means that the results cannot be pooled into meta-analyses to give a more accurate effect size. The lack of detail regarding the intervention practices (was touch used or not, for instance) makes it difficult to establish if direct contact has an impact on treatment outcome, or even if different studies are measuring the same intervention. Finally, the lack of detail given about the practitioners and their interaction with the participants makes it difficult to draw conclusions about the impact of these variables. This is especially important in view of the suggestion that the practitioner is a vital aspect of any healing practice.47Walach (2007). The issues can be addressed by researchers explicitly reporting these aspects of their research in study reports.
Despite finding a medium effect size for both physiological and psychological outcomes across study designs, even after removing low quality studies, the lack of detail within the studies led Peters to conclude:
… it is impossible to make substantive claims about the TT research base from this initial meta-analytic review … more rigorous research still needs to be done to establish a solid body of evidence that supports the effectiveness of TT as a nursing intervention.48Peters (1999).
Winstead-Fry and Kijeck conducted a meta-analysis of Therapeutic Touch studies conducted between 1979 and 1997. They searched through both bio-medical and psychology databases and conducted a library search to identify relevant doctoral dissertations. Their inclusion criteria were that studies used only the standardized method of TT; that papers be published research studies or doctoral dissertations; that the studies used human participants; and that they reported the means and standard deviations of both groups.
This search produced thirteen studies that fit the criteria for inclusion in the meta-analysis, which revealed a moderate significant effect of d =.39.
When reviewing the standard of the studies, Winstead-Fry and Kijeck concur with Peters that the demographics of participants are not sufficiently reported to allow for control of their possibly confounding effect. In particular, an ‘…inadequate presentation of exactly what researchers mean when they say they are following the Krieger-Kunz method’ makes it difficult to establish if the same intervention is being assessed across studies. Winstead-Fry and Kijeck also question the ecological validity of studies using healthy populations, and those in which the treatment time is limited to five minutes, the latter especially, given the suggestion by Krieger and Kunz that the average treatment time is twenty minutes. If interventions lack ecological validity it is not possible to generalize research findings to real life situations, limiting the application of the research results.
As with Peters, although this meta-analysis produced an overall moderate effect, the methodological weaknesses of the studies led Winstead-Fry and Kijeck to conclude that there is a need for more research on TT efficacy49Winstead-Fry & Kijeck (1999).
In their review of distant healing studies, Astin et al. found eleven studies investigating the effects of therapeutic touch, the average effect size of which was a moderate d = .63 (p = .003). All are subject to certain methodological weaknesses, which leads the researchers to advise their results be interpreted with caution. Like Peters and Winstead-Fry and Kijeck, Astin et al. conclude: ‘…additional studies of distant healing that address the methodological issues outlined … are now called for, to help resolve some of the discrepant findings in the literature and shed further light on the potential efficacy of these approaches.’50Astin, Harkness, & Ernst (2000).
Roe, Sonnex & Roxburgh found nineteen studies of TT that conformed to their inclusion criteria for meta-analysis, giving a medium effect size (r = 0.371). These results were heterogeneous, and three outliers had to be removed to render the results homogenous. Although the effect size decreased, it was still present (r = 0.276). Roe, Sonnex & Roxburgh also found that the study quality across all of the approaches was an issue, with significant correlations between effect size and randomization method, and suggestive correlations between effect size and control of extraneous variables, average quality rating and clear specification of planned analysis. However, after controlling for these aspects of methodological quality a small effect size (for all types of non-contact healing approaches) was still present (r = 0.115).51Roe, Sonnex, & Roxburgh (2015).
The findings of these reviews are, like those of IP, somewhat inconclusive; whilst they all show a moderate effect of TT, the issues around study design are raised by all the researchers and serve to reduce confidence in the strength of the results, despite evidence to show that quality only has a limited influence on effect size. It should also be noted that some researchers have criticized TT reviews and meta-analysis for insufficient quality assessment and cherry-picking favourable results.
Example of Sound Methodology
An example of a methodologically sound investigation in this area is by Meehan. She investigated the effects of TT on post-operative pain. One hundred and eight participants were randomly and blindly assigned to one of three equal sized groups (n=36 per group): TT, sham TT or standard intervention (drugs). The TT intervention was provided by three TT healers with at least two years’ experience. The sham TT was provided by seven nurses with no training in TT, who mimicked the hand movements of the genuine TT healers whilst silently counting backwards in sevens to prevent any inadvertent healing being administered. Both the genuine and the sham TT were limited to five minutes duration. Pain was measured by the pain visual analogue scale (VAS) pre- and one hour post-intervention. The VAS is a ten centimetre line, labelled at one end as ‘no pain’ and at the other end as ‘pain as bad as can be’, participants mark at which point on the line they feel their level of pain is. If TT or sham TT participants requested drugs in that one hour period it was noted, and their post-intervention score was marked as the same as their pre-intervention score. Nurses taking VAS measures were blind to participant allocation. Interventions occurred when participants asked for pain relief if it was twenty-four hours after their surgery and three hours after receiving pain medication.
Both TT and standard intervention groups showed a reduction in pain from pre-healing to post-healing; the sham TT group did not. The standard intervention group was found to be significantly more effective than TT (p =<.001) and TT was found to be more effective than sham TT though not significantly so (.05<p<.06). Whilst these findings do not support the use of TT in place of traditional pain relief, secondary analysis did find some evidence to suggest an effect of TT: although participants in both the TT and the sham TT groups requested pain relief, the number of participants in the TT group who did so was significantly smaller than those in the sham TT group (c2=4.73, p<.05) and those who did waited significantly longer to do so than those in the sham TT group (c2=4.69, p <.05). Meehan concluded that ‘TT may tentatively be classed as a mild analgesic: however it is not clear whether, or to what extent, the analgesic effects of TT are different from those of a placebo.’52Meehan (1993).
One strength of this study is that participants in both the TT and the sham TT conditions were blinded to their group allocation, and nurses who were collecting the pain data were also blinded, thus reducing the possible effect of placebo and expectancy. As Meehan noted in her conclusion, because the participants were aware that they were receiving an intervention that was not standard care, it is not possible to eliminate entirely the possibility of a placebo effect, the fact that the overall differences between the TT and sham TT group did not reach significance is further support for an argument of placebo effect.
The design of the sham condition is another methodological strength of this study. By mimicking the genuine intervention, the sham intervention gives us an idea of the possible placebo effects involved in TT, being administered by people with no training in the methods, and whose minds were occupied all ensure that no inadvertent healing was administered, which could have reduced the differences in outcomes between the groups. A further strength is that participants were blocked by baseline pain severity (that is, how much pain they were in at the beginning of the trial before receiving any interventions) ensuring that there were no significant differences between the groups that might have influenced the results.
Meehan clearly described both interventions in the research report, thus addressing some of the points of lack of description raised by Peters and Winstead-Fry and Kijeck. Exact demographics for each group were not reported, but Meehan did state that there were no significant demographic differences between the groups, suggesting that the differences found were down to artefacts. Unfortunately the limitation of the TT and sham TT interventions to five minutes does somewhat reduce the ecological validity of the study, and leads one to question how the results may have differed, had participants received the standard twenty-minute intervention as set out by Krieger.
Overall, the strengths of this study appear to outweigh the weaknesses. In his review of spiritual healing studies, Benor gave it the highest rating for quality, stating ‘this study is reasonably well designed considering the constraints of doing healing research in an American hospital at a time when healing still appeared strange to most medical authorities.’53Benor (2001).
Summary
TT seems to contain aspects of both allopathic and alternative medicine and has been widely researched within the academic nursing community. The research so far has been of variable quality and gives inconsistent results. However, a number of reviews have shown an overall positive effect, even after controlling for study quality, indicating the presence of an effect.
As with IP, further more rigorous research and reporting is required before there can be a definitive conclusion made as to the efficacy of TT.
Reiki & Johrei
Reiki and Johrei are discussed here in combination, as forms of healing that share common aspects. Both originate from Japan, and involve the projection of healing energy through the hands of the healer. In both methods this is understood to be an external, universal energy, as opposed to the personal reserve of energy utilized in TT. Likewise, both Reiki and Johrei practitioners understand the energy to be self-directing, and do not attempt to manipulate or influence its flow. Finally, a key similarity is that one must receive blessings or ‘attunements’ to be able to channel the healing energy. The processes and specific philosophies involved in each method will be presented, along with discussion of the advantages, drawbacks and empirical evidence for each.
Reiki
Reiki was introduced to the West in 1937 by Hawayo Takata (1900–1980), a student of Dr Chujiro Hayashi (1878–1940), who in turn had been taught by Dr Mikao Usui (1865–1926) who developed the system.54Singg (2004). Reiki is an energy-based healing intervention – ailments are believed to be associated with (though not necessarily caused by) imbalances and blockages in the energetic body. Reiki healing is administered by moving the hands over the body of the patient in a series of specific movements whilst channelling energy into the energetic body, or by channelling energy into the energetic body from a distance to restore balance to the energetic body.55Benor (2001); Singg (2004); VanderVaart, Gijsen, de Wildt, & Koren (2009).
The term reiki means universal life force or energy, which is believed to be channelled by the practitioner, through their hands or at a distance, during a healing session. Unlike TT, Reiki practitioners do not transmit their own energy to healees; rather, they claim to act as ‘conduits’ for the universal life energy that is believed to be in all things and capable of reaching the parts of the body where it is needed, without direction from the healer.56Singg (2004). This shows Reiki as a more holistic approach than TT, being not at all symptom driven. Again unlike TT, there is no assessment phase or attempt to ‘fix’ depletions or blockages of energy, which means practitioners do not need to know the client’s symptoms or diagnosis in order to administer an effective healing treatment.
Another difference is that Reiki is not taught in the traditional sense; rather, students receive ‘attunements’ from Reiki Masters. These attunements are believed to prepare the healers for channelling the universal energy. Reiki students are also given manuals showing the specific hand positions and gestures said to channel the flow of energy, and these are practised during classes.57Singg (2004).
There is no standardized curriculum for Reiki training, however there are three ‘levels’ of achievement which are universal within Reiki:
- Reiki I is laying-on of hands healing
- Reiki II is distant healing.
- Reiki III is an induction to Master level.58Benor (2001).
Training to the level of Reiki Master can involve anywhere between three and ten stages, depending on the training techniques andassociation of the Master who is teaching.59Singg (2004). The various hand positions used within a healing session can also vary according to the teacher. Such variation in teaching methods may lead to uncertainty regarding the validity of a single term to describe what could be a variety of practices. However, with regards to the hand positions used, Dr Usui, the founder of Reiki, argued that because the energy channelled during a session is intelligent and self-directing, it will go where it is most needed, regardless of the hand positions used.60Vitale (2007).
With regard to the number of stages that training is divided into, ‘ … the ultimate goal at every level is a series of attunements,’61Singg (2004). meaning that the main outcome of all teaching methods is the same. Dr Usui empowered sixteen Reiki masters in his lifetime, commenting that each appeared to be ‘empowered with individual gifts which may differ from those of other masters in subtle or substantial ways’.62Benor (2001). This accounts for the diversity in training techniques and emphasizes their shared lineage and underlying philosophies.
It can be concluded that the similarities within Reiki are more important than the differences. Reiki healers will all access the same theoretical ‘energy’ that is believed to be the ‘active ingredient’ of Reiki healing.
Benor believes that recent Reiki masters may not have been as selective as earlier Masters when offering level III attunements, resulting in Reiki masters with less experience or fewer abilities than in the past. He also criticizes the large sums of money charged for level III training, which may account for the lack of discrimination when offering this service.63Benor (2001).
Benor describes many strengths of the Reiki method of healing, as a holistic approach that encourages emotional and spiritual healing as well as physical. This holistic approach often extends to the practitioner, with some Masters encouraging their students to work on themselves to facilitate their healing abilities. Because the universal life force is considered to be intelligent, healers do not manipulate the energy or direct it in any way, meaning that healers’ own biases, or possible lack of knowledge regarding allopathic medicine, or the healee’s personal situation, cannot result in ineffective healing – all the more beneficial considering that Reiki training is open to anyone. Finally, Benor points out that many research studies have supported the efficacy of Reiki.64Benor (2001).
Evidence
Reiki healing has been investigated in a large number of papers, enough to necessitate reviews and meta-analysis that summarise their findings; these often include an appraisal of the calibre of the methodologies used.
Reviews and Meta-Analyses
Vitale conducted an integrative review of Reiki research. A mix of biomedical and nursing databases, Reiki organisational websites as well as the NCCAM (National Centre of Complementary and Alternative Medicine) website were searched to find relevant data. To be included in the review, papers had to be English-language, clinical-trial research that used human samples and random assignment to either a Reiki intervention or placebo/control group. Sixteen papers in total met the inclusion criteria, which were grouped for review by study area, the results of which are shown in Table 2:65Vitale (2007).
Table 2: Results of Vitale

* One of the studies used Reiki in conjunction with other complementary and alternative medicine modalities so the impact of the Reiki intervention alone could not be established.
Although Vitale did not measure study quality empirically, she does state that methodological issues exist within the studies included in the review similar to those identified in other reviews and meta-analyses of spiritual healing research. These include lack of sufficient blinding and randomization, insufficient sample sizes, lack of detail regarding intervention protocol, insufficient control of extraneous variables or interaction effects, and lack of placebo/control conditions.66Vitale (2007).
VanderVaart, Gijsen, de Wildt and Koren conducted a systematic review of the empirical evidence for Reiki.67VanderVaart, Gijsen, de Wildt, & Koren (2009). They searched Medline, EMBASE, the Cochrane Library and Google Scholar for relevant studies. To be included in the review, studies had to include both a test group and a control group, and use human participants; also, the intervention had to be administered by a Reiki healer, and studies had to be published in English prior to December 2008. VanderVaart et al. subjected the eligible studies to quality assessment of both their methodology and their reporting. Twelve studies in total fitted the criteria and were included in the analysis.
In their analysis of reporting quality, VanderVaart et al. found that randomization, concealment and group allocation (important features when trying to establish a placebo/expectancy effect) were not reported adequately. Only eight of the studies adequately reported their primary outcome measure. It is important for researchers to establish their primary outcome measure a priori, lest they be accused of cherry picking results when a number of outcome measures are reported, as is the case here: between twelve studies, thirty-one different outcome measures were reported. VanderVaart et al. emphasise the importance of explicit, detailed reporting in the field; ‘In order to be accepted as true scientific evidence, adequate reporting of future Reiki RCTs or mixed methods RCTs is crucial. Of the items that were not reported adequately, all of them were reported adequately in at least one study, indicating that it is possible to report adequately.’68VanderVaart, Gijsen, de Wildt, & Koren (2009). In their analysis of methodological quality, eleven of the papers received a ‘poor quality’ rating on the Jadad scale; only the one remaining study was rated as ‘good quality’. This lack of methodological rigour makes it difficult to draw definitive conclusions about the efficacy of Reiki, as the possible effect of placebo and other influences cannot be eliminated.
Nine of the twelve studies reported significant outcome measures in favour of the Reiki intervention on at least one outcome measure. The remaining three reported no significant differences between the groups. None of the studies reported negative findings. VanderVaart et al. concluded: ‘based on the poor quality of studies and their reporting, it is currently impossible to draw definitive conclusions about the efficacy of Reiki.’69VanderVaart, Gijsen, de Wildt, & Koren (2009).
Lee, Pittler and Ernst conducted a review of RCTs investigating the efficacy of Reiki. They searched 23 British, American, Korean, Chinese and Japanese databases to identify relevant studies.70Lee, Pittler, & Ernst (2008). The inclusion criteria were that studies used non-healthy human participants, compared a Reiki intervention with a control group, measured efficacy by a clinical outcome measure and reported statistical results. Once identified, studies were subject to quality assessment using the Jadad scale. Nine studies were included in the review. Studies ranged in quality from two to five out of a possible five. The average quality score was 3.1 which is considered ‘good quality’. Whilst this is an improvement on the scores seen in the Vandervaart review, it still shows a lack of high quality studies and allows for the possibility of outside influences.
Only four of the studies described their randomization processes, five reported blinding, and only two reported allocation concealment methods – a similar lack of detail as found by VanderVaart. This lack of information means that, like the Vandervaart review, ‘it is therefore impossible to tell to what extent the therapeutic response (if any) is due to specific or non-specific effect.’71Lee, Pittler, & Ernst (2008).
The studies reported a mix of non-significant results and significant results in favour of Reiki, across a number of different outcome measures. These conflicting results, combined with the methodological and reporting issues within the studies, lead Lee et al. to conclude ‘the evidence is insufficient to suggest that Reiki is an effective treatment for any condition. Therefore the value of Reiki remains unproven.’72Lee, Pittler, & Ernst (2008).
The state of the evidence for the efficacy of Reiki as a therapeutic intervention is similar to other approaches to healing: whilst the research suggests that there is some effect, the lack of methodological rigour and inadequate detail in research reports means that no definitive conclusions can be reached.
Example of Sound Methodology
Are any Reiki studies conducted well and reported in adequate detail? Of the four using human participants reviewed by Benor, none received an ‘excellent’ rating for quality; two received a rating of IV (‘critical elements are missing’) and the remaining two received a rating of III (‘reporting of details is seriously deficient’).73Benor (2001). This suggests that the lack of both methodological rigour and explicit reporting is endemic to Reiki research. However, Benor’s review does not include a study by Shore, which appears to be a methodologically rigorous study.74Shore (2004).
Shore investigated the effect of Reiki on depression and stress. Forty-five participants who required treatment for depression and stress symptoms were randomly assigned to either the hands-on Reiki (thirteen participants), distance Reiki (sixteen participants) or distance Reiki placebo conditions (sixteen participants). Participants in the distance Reiki condition were blinded and participants in the hands-on and placebo distance Reiki groups were deceived into thinking they were either receiving mock Reiki (in the case of the hands on group) or actual distance Reiki (in the case of the distance Reiki placebo group). Reiki treatments were provided by twelve Reiki Masters; participants received 1-1.5 hours of Reiki per week for six weeks. To ensure ecological validity, participants – regardless of group – all had their sessions in a healing setting. Placebo healing participants were at a different, but similar, location to the one used in genuine healing groups, to prevent ‘linger’ effect. Outcomes were measured using the Beck depression inventory scores (BDI), Beck hopelessness scale (BHS) and the perceived stress scale (PSS), which were taken at baseline, post treatment and at one year follow up. The two treatment conditions showed significantly improved scores compared to the placebo condition on all scales (Hands on Reiki vs. Placebo: BDI t –2.0, p =.05η2= .09, BHS t =-2.40, p =.02η2=.12 and PSS t =-3.03η2=.018, p =.004. Distance Reiki Vs. Placebo: BDI t –3.01, p =.004,η2=.018, BHS t =-2.65, p =.01, η2=.14 and PSS t =-2.93, p =.005, η2=.17.)
This was the same one year on. The placebo group were offered Reiki treatment after the follow up data had been collected and were asked to complete the outcome measures after their treatment. They showed significantly improved scores post treatment (BDI p =<.0001, BHS p =.010 and PSS p =.002).
This study provides strong evidence in support of Reiki as a form of healing: both types of Reiki resulted in significant improvement in participants’ well-being, and the fact that only the actual treatment group showed improvement – although both groups believed they were receiving treatment – counters arguments of placebo or expectancy effect. This also means that the lack of improvement in the placebo group prior to treatment cannot be attributed to chance. In addition, the study includes a long-term follow-up component, often neglected research.
This study was included in all three of the review papers discussed previously, and so does suffer from some of the drawbacks discussed in those reviews. However, most of these criticism are directed at the reporting of study design rather than methodology. Criticisms have been made regarding the clinical significance of the small effect sizes found, the limited generalizability due to the small sample size, and the lack of clarity regarding the concealment methods. Despite these flaws, Lee et al. scored this study three out of five or ‘good quality’ on the Jadad scale.75Lee, Pittler, & Ernst (2008). VanderVaart scored it only a two, or ‘poor quality’, on the Jadad scale.76VanderVaart, Gijsen, de Wildt, & Koren (2009).
As Lee et al. do not report a breakdown of their Jadad scores for each study included in their review, it is difficult to identify the discrepancies between the two scores. It is possible however to identify one discrepancy between the scores given by VanderVaart for the Jadad scale and for the CONSORT scale they used to assess quality of reporting. In the Jadad scale, VanderVaart awarded the Shore paper a 0 for the item ‘was the study described as double blind?’ meaning it was not. However, they answer both question 11 and 11b of the CONSORT criteria (‘were participants blinded?’ and ‘was the assessor blinded?’) with ‘yes’. According to the Jadad scale, ‘the method will be regarded as appropriate if it is stated that neither the person doing the assessments nor the study participant could identify the intervention being assessed…’77Jadad et al. (1996). Shore explains that participants were blind to treatment allocation and were deceived into believing they were in receipt of a different intervention than the one they were receiving and that a placebo distance Reiki condition was used. All this means the blinding item on the Jadad scale should have been scored 1, while item 5 of the Jadad scale (as long as in item 2 the method of double blinding was appropriately described – identical placebo, active placebo, dummy, etc.) should have been scored a 1.
This suggests that, of the twelve items on the CONSORT scale that VanderVaart answered with ‘no’, three could in fact be answered with a ‘yes’ or ‘partly addressed’:
- Participant’s settings and locations: Shore describes the features of the rooms in which the healing takes place but not the locations.
- Recruitment: Shore states where recruitment posters were placed, describes the elimination criteria for volunteers and explains that participants were randomly selected from the pool of eligible volunteers.
- Overall evidence: Shore used three different outcome measures (established a priori) so scores could not be pooled to give one overall outcome measure, however the results are summarized concisely within the conclusion.
VanderVaart et al. make the fair assessment that the details of randomization and allocation, success of blinding, participant flow, intention-to-treat analysis and sample size determination were not adequately addressed within the report. Overall, however, it seems that their assessment of the quality of this paper is somewhat inaccurate, leading to a lower quality score than is justified, especially given the higher quality ratings given by other researchers reviewing this paper.78Vitale (2007); Lee, Pittler, & Ernst (2008). Most criticisms of this paper centre on the reporting rather than methodology. However, this is a prime example however of how poor reporting can undermine confidence in results from an otherwise rigorous study.
Summary
Following an emerging pattern within healing research, the evidence provided by studies of Reiki is suggestive of some effect; however the poor methodological quality of those studies or lack of detail within reports, or a combination of both, means that no conclusions can be drawn regarding the efficacy of Reiki as a clinical intervention. Further, more rigorously designed and explicitly reported research is necessary before a true effect of Reiki can be established.
Johrei
Johrei is a less well known form of healing, with fewer research studies investigating its efficacy than Reiki. It is just one aspect of an entire philosophy of living that originated in Japan, developed by Mokichi Okada in the 1920s.79British Johrei Society (2005-2010). According to this philosophy, what occurs in the spiritual body is reflected in the physical body and vice versa. Followers of Johrei see physical illness or psychological suffering as a reflection of the purification process that occurs in the spiritual body, when ‘clouds’ caused by negative words, actions, thoughts, or physical pollutants become too ‘dense’ and need to be eliminated.80British Johrei Society (2005-2010); Johrei Fellowship (2002). The act of Johrei healing aids this elimination process by helping to purify the spiritual body through the transmission of divine light through the palm of the administrator to the body of another person. To be able to practise Johrei, one must undergo a basic or foundation course and receive the ‘Ohikari’, meaning sacred focal point. This allows one to receive the Divine light of purification and to channel it, rather like the ‘attunements’ one receives at each of the three levels of Reiki training.81https://johreicentreuk.blogspot.com/p/johrei.html
There is little information about what precisely is involved in the basic courses offered, or how homogenous the teaching is among the various providers. A Johrei healing session customarily involves the healer and healee facing each other, whilst the healer points their cupped palm towards the upper body of the healee: it is believed that the Divine light of purification is channelled through the hand of the healer to the healee.82Laidlaw et al. (2006); Reece, Schwartz, Brooks, & Nangle (2005).
Because the aim of Johrei is not to ‘cure’ specific illnesses, but rather to purify the whole spiritual body, practitioners do not manipulate the energy or direct it in any way. This is a strength of Johrei healing, because it means that (as with Reiki) the biases of the healers – or their possible ignorance regarding allopathic medicine or the healee’s psychological state – need not result in diminished healing efficacy. This is especially important, considering that Johrei training, as with Reiki, is open to anyone.
Another strength of Johrei is that it is a holistic approach, considering emotional and psychological difficulties/illnesses, like physical illnesses, to be a result of the purification of ‘clouds’ from the spiritual body. This means that like Reiki, and unlike TT, these aspects of well-being are not neglected or ignored in favour of treating physical ailments only: the transmission of divine light helps to restore balance to the person as a whole. A further strength of Johrei is that research has shown that those who administer Johrei benefit from increased well-being as well as the healees.83Reece, Schwartz, Brooks, & Nangle (2005).
The Johrei philosophy takes elements from Christian and Buddhist beliefs as well as traditional Chinese philosophy. Within Johrei, it is believed that Satan exists, and that he has the power to influence people’s lives in a negative way. The Christian concept of the judgement day is also accepted within Johrei, with Johrei healing seen as a way to become ‘purified’ in preparation for judgment. It is also believed that the divine light transmitted during Johrei healing is the same energy that was used by the Bodhisattva Cintamani-cakra Avalokitesvara to bless people in times of need. Johrei also uses the traditional Chinese philosophical concepts of Yin and Yang, believing the spirit to be associated with Yang and the body with Yin. It is this combination of both elements that makes us human and it is important to acknowledge them when treating people.84Jinsai.org.
Evidence
The practice of Johrei healing has been the subject of fewer research studies than the other forms of spiritual healing discussed previously. A single meta-analysis has been carried out in combination with Reiki85Roe, Sonnex, & Roxburgh (2015). which means that the effects of Johrei alone cannot be judged in isolation. However, there is sufficient research to give indications of whether or not there is an effect, and the quality of this work can also be assessed.
Reece, Schwartz, Brooks and Nangle researched the effects of Johrei on the well-being of both healers and healees.86Reece, Schwartz, Brooks, & Nangle (2005). Two hundred and thirty six participants took part, filling out the Johrei subjective experience scale, which measures emotional states, and the Arizona Integrated Outcomes Scale, a measure of well-being, before and after giving or receiving a session of Johrei. Healees ( n = 150) reported a significantly greater decrease in emotional distress than the healers(n = 86) (F [1,234] = 8.968, p =<.003). Both healers and healees reported significant increases in positive emotional state (F[1,234]=178.93, p =,.001), with the increase in positive emotional state in the healers being significantly higher than that of the healees (F[1,234]=4.786, p =<.003). The same was seen in the overall well-being scores (F[1,228]=207.48, p =<.001 and F[1,228] = 6.047, p =<.015 respectively).
This study provides some evidence to support the claims of Johrei to be an effective form of healing. Healees showed a greater reduction in negative state than healers, their pre-intervention distress scores being higher than those of the healers, suggesting that Johrei may be more effective for worse conditions. However, as this study lacked a control or sham condition it is possible that the findings are the result of placebo or expectancy effects, especially considering that all participants were recruited from a Johrei centre.87Reece, Schwartz, Brooks, & Nangle (2005).
Brooks, Schwartz, Reece and Nangle conducted research into the effects of Johrei on substance abuse recovery.88Brooks, Schwartz, Reece, & Nangle (2005). Participants were twenty-one people in a residential rehabilitation programme, twelve of whom were randomly assigned to receive three twenty-minute sessions of Johrei per week for five weeks from a number of practitioners. The remaining nine were assigned to a waiting list control group. The outcome measures were the Johrei subjective experience scale, which measures experiences that have been commonly associated with Johrei, and the Arizona Integrated Outcomes Scale, a holistic measure of well-being. These scales were completed before and after every healing session. Measures of life problems, substance cravings, mood, and adherence to twelve-step recovery programmes were administered after the five week intervention period. During the intervention period, positive emotional state, energy and well-being showed significant improvement for the Johrei group compared to the control group (t =-7.49, p =<.001, t =-5.38, p =<.001, and t =-13.6, p = <.001 respectively), whilst stress/depression and physical discomfort showed significant decrease ( t =12.71, p =<.001 and t =6.29, p =<.001 respectively). After the intervention, depressive symptoms, traumatic symptoms, externalising behaviours, vigour and practice of the twelve steps showed significantimprovement for the Johrei versus control group (due to the small sample size significance was set at p =<.01) (F (1,17) = 8.20, p – <.011, F (1,17) = 3.26, p =<.089, F (1,17) = 3.14, p =<.093, F (1,17) = 4.52, p =<.048 and F (1,18) =7.09, p <.016 respectively).
This study provides some evidence for the efficacy of Johrei as a healing intervention, showing Johrei to have an impact not only on well-being and emotional states but also on adherence to twelve-step recovery programmes. However, being a pilot study the sample size was small and the significance level lower than in conventional studies. It also suffers from lack of blinding and placebo control, which means the results could be caused by placebo or expectancy effects.
Gasiorowska et al. investigated the effects of Johrei on chest pain not caused by cardiac problems.89Gasiorowska et al. (2008). Thirty-nine participants completed a baseline diary of chest pain frequency and severity for two weeks (participants had to experience three episodes per week to be eligible for the trial) as well as scales measuring demographics, symptoms, stress and anxiety. Participants were randomly allocated to either the intervention (n=21) or wait list control (n=18) group. A two-week diary was completed by participants at the end of the study period, as was the quality of life scale. Participants in the intervention group received eighteen twenty minute sessions of Johrei treatment over six weeks. As patients in the intervention group saw the practitioner, and those in the control group did not, there was no blinding. The Johrei group showed significantly reduced symptom intensity after treatment (20.28 vs. 7.0, P = 0.0023 (23.06 vs. 20.69 respectively, P = N.S), while the control group did not. (23.06 vs. 20.69 respectively, P = N.S). No other statistically significant differences were identified between the groups.
This study also provides evidence to support the efficacy of Johrei healing; however without a placebo or sham control group it is not possible to eliminate placebo or expectancy effects.
These examples demonstrate that, as with the Reiki research, although there does appear to be a trend of evidence to support the effects of Johrei healing, much of the research suffers from methodological flaws that make it difficult to eliminate the possibility of outside influences or placebo effect affecting the results.
Example of Sound Methodology
One of the more methodologically rigorous studies into Johrei is that conducted by Laidlaw et al.90Laidlaw et al. (2006). They investigated the effects of Johrei on laboratory stress. Thirty Three participants took part. The study used a counterbalanced crossover design, with participants acting as their own controls. Participants were randomly assigned, on a double blind basis, to receive the Johrei intervention after either completing a laboratory stressor task for the first time or for the second time. As a stressor Laidlaw utilised the Paced Auditory Serial Addition Task (PASAT), which is described as
… an auditory recording of a series of 70 single digit numbers paced so that each number is presented at 3-s intervals followed by a further 70 digits paced 2-s apart. The participants must add the last two numbers heard, while ignoring the distraction of the sum that s/he has said aloud.91Laidlaw et al. (2006).
Participants completed the PASAT task and then completed ten minutes of either receiving Johrei healing (intervention condition) or sitting quietly (the control condition) after which point saliva samples were taken and mood questionnaires completed. After a rest period of thirty minutes, participants again completed the PASAT task, followed by ten minutes of the intervention or sitting quietly. Participants did this twice; the first time was to acclimatise them to the laboratory environment, so that when the data was taken during the second visit, it was not influenced by possible additional stress caused by being unfamiliar with the procedure or environment.
During the Johrei intervention, participants sat in a chair with their eyes closed and one of three experienced Johrei practitioners administered Johrei from behind, without touching the participants. During the control conditions, the practitioner still sat behind the participant but did not administer Johrei. Stress hormone levels showed no significant differences between Johrei and control conditions (cortisol z = 1.14, p =ns, DHEA z =1.10, p =ns and IgA z = .93 p =ns) but the Johrei intervention did have a significant positive effect on mood when compared to control condition (F (1,32)=8.35, p =.007).92Laidlaw et al. (2006).
This study lends support to the efficacy of Johrei as a healing intervention. Although no physical changes were manifest, the changes in mood resulting from the Johrei intervention show an improvement in well-being. This is a well-conducted study, with controls for the added stress of being in a laboratory environment and double blind measures to counteract any placebo/expectancy/bias arguments.
Summary
Overall, the evidence for Johrei is similar to the other forms of spiritual healing discussed. There is evidence to suggest that Johrei does have a healing effect, however methodological issues – lack of placebo, sham or even control conditions, small sample sizes, and lack of blinding – mean that alternative counter-hypotheses cannot be ruled out.
Summary of Johrei and Reiki
Roe, Sonnex & Roxburgh conducted a meta-analysis of seven studies of Reiki and Johrei.93Roe, Sonnex, & Roxburgh (2015). They found a medium effect size (r=0.320). The results suffered from heterogeneity, but the removal of one outlier rendered the results homogenous. This reduced the effect size, but it was still present (r= 0.224). Roe, Sonnex & Roxburgh found that the study quality across all of the approaches was fairly low, and that some correlations between methodological quality and effect size were significant or suggestive. When these aspects of methodological quality were controlled for, a small effect size for all types of non-contact healing approaches (not just Reiki and Johrei) remained (r= 0.115).
As has been shown in the research into other forms of spiritual healing, there is evidence to suggest that both Reiki and Johrei have a tangible effect on health and well-being, however these findings are tempered by poor methodological rigour and poor reporting of study design, which appears to be almost inherent within this research.
Idiosyncratic/Other Types of Healing
There are a number of studies of unspecified methods: ‘spiritual healing’,94Sundblom, Haikonen, Niemi-pynttari, & Tigerstedt (1994); leGallez, Dimmock, & Bird (2000). ‘healing with intent’,95Bunnell (2002). ‘distant healing intent’,96Radin, Machado, & Zangari (1998). and so forth. These studies have been grouped together under the term ‘idiosyncratic’ healing, as they tend to lack an established framework or philosophy. Most idiosyncratic healers understand their healing to work from an ‘energy medicine’ perspective, sending ‘healing energy’ or ‘healing intentions’ to the healee.97Sundblom, Haikonen, Niemi-pynttari, & Tigerstedt (1994); leGallez, Dimmock, & Bird (2000); Radin, Machado, & Zangari (1998); Dixon (1998); Loveland-Cook, Guerrerio, & Slater (2004). The ‘transmission’ of the energy or intentions can vary, sometimes being projected from the hands98leGallez, Dimmock, & Bird (2000); Dixon (1998); Loveland-Cook, Guerrerio, & Slater (2004). and sometimes being an act of will on the part of the healer.99Radin, Machado, & Zangari (1998); Beutler et al. (1988).
Evidence
A large amount of research has been carried out with healers not affiliated with any specific tradition. Whilst some of this research has been included in reviews and meta-analysis, it has generally been analysed together with data from studies of other, more standardized forms of healing such as TT and Reiki. This means the impact of idiosyncratic forms of healing alone cannot be established. However, in their review of distant healing studies, Astin et al. reviewed seven studies that they labelled as ‘other distant healing’. This group included studies of ‘distance or distant healing’, ‘paranormal healing’ and ‘remote mental influence’, amongst others. Of these seven trials, four showed significant positive results in favour of the healing intervention, while the remaining three showed no significant differences between the groups.Five of the seven studies could be included in effect size analysis, which showed an average effect size of d=.38 (p = .073). Astin et al. identified certain methodological weaknesses within all of the studies they reviewed, leading them to recommend prudence when drawing inferences from the findings.100Astin Harkness, & Ernst (2000).
Roe, Sonnex & Roxburgh conducted a meta-analysis of idiosyncratic healing. Twenty studies conformed to their inclusion criteria, giving a small effect size (r=0.163). The results displayed significant heterogeneity, and three outliers had to be removed to make the results homogenous. This increased the effect size (r= 0.193). Roe, Sonnex & Roxburgh found that the study quality across all of the approaches was fairly low, with correlations between effect size some aspects of methodological quality. However, even after controlling for these quality aspects a small effect size (for all types of non-contact healing approaches) remained (r= 0.115).101Roe, Sonnex, & Roxburgh (2015).
Example of Sound Methodology
Bunnell conducted research into the effects of ‘healing with intent on asthma’. Forty eight participants took part, twenty-two with asthma and twenty-six without. Peak flow measures were taken after each session. In the first session, participants received ten minutes of healing. In the next session one week later, they received sham healing (the healer was present but did not try to administer healing and instead read an article without the participants’ knowledge). Genuine healing involved the healer sitting behind the participant and entering a meditative state which is believed to affect the participant. The study was conducted double blind, meaning that participants did not know when they were receiving genuine healing and when they were receiving sham healing, and neither did the researchers. The non-asthmatics showed no significant differences in peak flow scores after receiving healing, or when healing results were compared to the sham control results. The asthmatics showed a significantly improved peak flow after the administration of healing (p=.009), which continued to be present after one week (p=.003). Peak flow performance did not improve more after the control session.102Bunnell (2002).
The results of this study lend support to the efficacy of spiritual healing for those with an illness. The asthmatic participants showed an improvement, while the non-asthmatics did not. This is an interesting result and suggests that if healing does work, it does so by specifically healing illnesses rather than by boosting health in general; otherwise one would expect to see an improvement in the results of the non-asthmatic participants also. The double blind aspect means that expectancy, bias and placebo effects are minimized and are unlikely to be responsible for the results. That the healer was occupied during the sham healing sessions means also that it is unlikely that any inadvertent healing occurred (though this would only serve to reduce the differences found if it had happened).
Studies of Healing Effects on Non-Human Samples
In their meta-analysis of non-contact approaches to healing, Roe, Sonnex & Roxburgh also looked at studies that used samples other than human – plants, animals and cells in vitro – which are not susceptible to placebo and expectancy effects.
All of the studies were classified as utilizing an idiosyncratic approach. Forty-nine studies conformed to their inclusion criteria, giving a small to medium effect size (r=0.258). As with the human studies, the results displayed significant heterogeneity, and ten outliers had to be removed to make the results homogenous. This reduced the effect size (r= 0.236), but not to the point of non-significance. They found that the study quality across all of the approaches was fairly low, with correlations between effect size and some aspects of methodological quality. However, even after controlling for these quality aspects a small effect size (for all types of non-contact healing approaches, across all samples, human and non-human) remained (r= 0.115).103Roe, Sonnex, & Roxburgh (2015).
Summary
Although the title of idiosyncratic healing is given to a mix of different approaches, the results of research into this type of healing have similar outcomes not only to other studies of idiosyncratic types of healing, but also to the other types of healing discussed here. The results are inconclusive, with some studies providing evidence for an effect and some not. Here too there is evidence of methodological weaknesses, such as lack of statistical power, lack of placebo or control condition and inadequate sample sizes. However, the meta analysis by Roe, Sonnex and Roxburgh suggests that these inadequacies are not enough to negate the effect seen.104Roe, Sonnex, & Roxburgh (2015).
Summary of All the Evidence
Multiple reviews into the major forms of healing have led to the same conclusion. Despite finding a small to moderate significant effect of healing interventions, poor methodology or poor reporting, or a combination of the two, means that no definitive conclusions can be drawn and that further more rigorous and well reported research is needed.
IP is the most widely practised form of spiritual healing and the method that has inspired the most research, has resulted in evidence to suggest a small effect.105Roberts, Ahmed, Hall, & Davison, (2009); Levin (2011). As stated, methodological weaknesses such as insufficient randomisation, blinding and concealment and inadequate controlling for influencing factors all serve to reduce confidence in the results found. However, meta-analyses provide evidence to suggest that these methodological issues do not influence the effect size sufficiently to render IP ineffective.106Astin, Harkness, & Ernst, E. (2000); Roe, Sonnex, & Roxburgh (2015). The inclusion of the concept of deity within IP further is a complicating factor with regard to arguments that spiritual healing should not be researched because of its ‘impossible’ mechanism.107Andrade & Radhakrishnan (2009); O’Mathúna et al. (2002).
Therapeutic touch could possibly counter those arguments, given its grounding in allopathic medicine. As with IP, there has been much research into TT, and this has generally provided evidence to support its efficacy.108Peters (1999); Winstead-Fry & Kijeck (1999). The methodological weaknesses seen in IP research are also present in many of the TT studies, although here too, meta-analyses have shown that these weaknesses alone are not enough to fully explain the impact of TT interventions.109Astin, Harkness, & Ernst, E. (2000); Roe, Sonnex, & Roxburgh (2015).
Research of both Reiki and Johrei has also produced findings that support their efficacy, although the results of the Reiki studies tend to be more mixed than those of Johrei.110Vitale (2007); VanderVaart, Gijsen, de Wildt, & Koren (2009); Lee, Pittler, & Ernst (2008); Reece, Schwartz, Brooks, & Nangle (2005); Brooks, Schwartz, Reece, & Nangle (2005); Gasiorowska et al. (2008).
Within Reiki research, the methodological weakness common in spiritual healing research seem particularly inherent: in Benor’s review of spiritual healing studies, the highest quality rating given to Reiki research was three out of a possible five.111Benor (2001). It would be of interest to examine whether this acute lack of methodological rigour in Reiki research has an influence on the results, especially considering that the rigorous study conducted by Shore produced strong evidence in favour of a healing effect.112Shore (2004). This issue is also seen within Johrei research, which commonly suffers from similar methodological weaknesses. Again, the meta-analysis by Roe, Sonnex and Roxburgh suggests that controlling for these issues does not negate the effects demonstrated in the research.113Roe, Sonnex, & Roxburgh (2015).
As with Reiki, studies of idiosyncratic healing approaches have shown mixed results and methodological weakness that could result in artefacts. The effect found in non-contact healing – in non-human samples not susceptible to placebo or expectancy effects – and the fact that controlling for methodological weakness does not eradicate the results seen, suggest that methodological weakness is not a full explanation of the effects. Nevertheless, it is vital that future studies be of rigorous methodological design, so that assertions of the impact of such interventions can be made with full confidence.
Charmaine Sonnex
Literature
Andrade, C., & Radhakrishnan, R. (2009). Prayer and healing: A medical and scientific perspective on randomized controlled trials. Indian Journal of Psychiatry 51/4, 247-53.
Astin, J.A., Harkness, E., & Ernst, E. (2000). The efficacy of ‘distant healing’: A systematic review of randomised trials. Annals of Internal Medicine 132/11, 903-10.
Benor, D.J. (2001). Spiritual Healing: Scientific Validation of a Healing Revolution. USA: Vision Publications.
Benson, A., et al. (2006). Study of the therapeutic effects of intercessory prayer (STEP) in cardiac bypass patients: A multicentre randomized trial of uncertainty and certainty of receiving intercessory prayer. American Heart Journal 151/4, 934-42.
Beutler et al. (1988). Paranormal healing and hypertension. British Medical Journal 296, 1491-94.
Borenstein, M., Hedges, L.V., Higgins, J.P., & Rothstein, H.R. (2009). Introduction to Meta-Analysis. West Sussex, UK: John Wiley & Sons.
British Johrei Society (2005–2010). What is Johrei? [Web Page preserved on Internet Archive.]
Brooks, A., Schwartz, G.E., Reece, K., & Nagle, G. (2005). Positive well-being changes associated with giving and receiving Johrei healing. The Journal of Alternative and Complementary Medicine 11/3, 455-57.
Bunnell, T. (2002). The effect of ‘healing with intent’ on peak expiratory flow rates in asthmatics. International Journal of Subtle Energies and Energy Medicine 31/1, 75-89.
Byrd, R. (1988). Positive therapeutic effects of intercessory prayer in a coronary care unit population. Southern Medical Journal 81/7, 826-29.
Cha, K., Wirth, D.P., & Lobo, R. (2001). Does prayer influence the success of in vitro fertilization-embryo transfer? Report of a masked, randomized trial. Journal of Reproductive Medicine 46/9, 781-87.
Cohen, C.B., Wheeler, S.E., Scott, D.A., Edwards, B.S., & Lusk, P. (2000). Prayer as therapy: A challenge to both religious belief and professional ethics. Hastings Centre Report 30/3, 40-47.
Dixon, M. (1998). Does ‘healing’ benefit patients with chronic symptoms? A quasi-randomized trial in general practice. Journal of the Royal Society of Medicine 91, 183-88.
Dossey, L. (1993). Healing Words: The Power of Prayer and the Practice of Medicine. USA: Harper Paperbacks.
Flamm, B. (2004). The Columbia University ‘miracle study’: Flawed and fraud. Skeptical Inquirer 28/5 (October).
Gasiorowska, A., et al. (2008). Clinical trial: The effect of Johrei on symptom of patients with functional chest pain. Alimentary Pharmacology and Therapeutics 29, 126-34.
Halperin, E.C. (2001). Should academic medical centres conduct clinical trials of the efficacy of intercessory prayer? Academic Medicine, 76/8, 791-97.
Harris, W.S., Gowda, M., Kolb, J.W., Strychacz, C.P., Vacek, J.L., Jones, P.G. & McCallister, B.D. (1999). A randomized, controlled trial of the effects of remote intercessory prayer in outcomes in patients admitted to the coronary care unit. Archives of Internal Medicine 159, 2273-78.
Hodge, D. (2007). A systematic review of the empirical literature on intercessory prayer. Research on Social Work Practice 17, 174-87.
Jadad, A.R., Moore, R.A., Carroll, D., Jenkinson, C., Reynolds, D.J., Gavaghn, D.J., & McQuay, H.J. (1996). Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Controlled Clinical Trials 17/1, 1-12.
Johrei Centre, Izunomi Kyodan United Kingdom. (n.d.). [Web page.]
Johrei Fellowship (2002). A Johrei lifestyle [Web Page preserved on Internet Archive.]
Jonas, W.B., & Linde, K. (2002). Conducting and evaluating clinical research in complementary and alternative medicine. In Principles and Practice of Clinical Research (1st ed.), ed. by J. Gallin, 401-26. New York: Academic Press.
Kreiger, D. (1975). Therapeutic touch: The imprimatur of nursing. American Journal of Nursing 75/5, 784-87.
Laidlaw, T.M., et al. (2006). The influence of 10 minutes of the Johrei healing method on stress. Complementary Therapies in Medicine 14, 127-32.
Lee, M.S., Pittler, H., & Ernst, E. (2008). Effects of Reiki in clinical practice: A systematic review of randomised clinical trials. International Journal of Clinical Practice 62/6, 947-54.
leGallez, P., Dimmock, S. & Bird, H.A. (2000). Spiritual healing as adjunct therapy of rheumatoid arthritis. British Journal of Nursing 9/11, 395-700.
Levin, J. (2011). Energy healers: Who they are and what they do. EXPLORE: The Journal of Science and Healing 7/1, 13-26.
Loveland-Cook, C.A., Guerrerio, J.F., & Slater, V.E. (2004). Healing touch and quality of life in women receiving radiation treatment for cancer: A randomized controlled trial. Alternative Therapies 10/3, 34-41.
Masters, K.S. (2005). Research on the healing power of distant intercessory prayer: Disconnect between science and faith. Journal of Psychology and Theology 33/4, 268-77.
Masters, K.S., Spielmans, G.I. & Goodson, J.T. (2006). Are there demonstrable effects of distant intercessory prayer? A meta analytic review. Annals of Behavioural Medicine 32/1, 21-26.
Meehan, T.C. (1993). Therapeutic touch and postoperative pain: A Rogerian research study. Nursing Science Quarterly 6/2, 69-78.
O’Mathúna, D.P., Pryjmachuk, S., Spencer, W., Stanwick, M., & Matheisen, S. (2002). A critical evaluation of the theory and practice of therapeutic touch. Nursing Philosophy 3/2, 163-76.
Pande, P.N. (2000). Editor’s correspondence. Archives of Internal Medicine, 160/12, 1873-74.
Paul, G. (2008). The remote prayer delusion: Clinical trials that attempt to detect supernatural intervention are as futile as they are unethical. Journal of Medical Ethics, 34/9, n18.
Peters, R.M. (1999). The effectiveness of therapeutic touch: A meta-analytic review. Nursing Science Quarterly 12/1, 52-61.
Powell, L.H., Shahabi, L., & Thoresen, C.E. (2003). Religion and spirituality: Linkages to physical health. American Psychologist 58/1, 36-52.
Pumpkin Hollow Farm. (2004). Therapeutic touch defined. [Web page preserved on the Internet Archive.]
Radin, D.I., Machado, F.R., & Zangari, W. (1998). Effects of distant healing intention through time and space: Two exploratory studies. Subtle Energies and Energy Medicine 113/207, 239.
Reece, K., Schwartz, G.E., Brooks, A.J., & Nangle, G. (2005). Positive well-being changes associated with giving and receiving Johrei healing. The Journal of Alternative and Complementary Medicine 11/3, 455-57.
Roberts, L., Ahmed, I., Hall, S., & Davison, A. (2009). Intercessory prayer for the alleviation of ill health. Cochrane Database of Systematic Reviews.
Roe, C.A., Sonnex, C., & Roxburgh, E.C. (2015). Two meta-analyses of noncontact healing studies. EXPLORE: The Journal of Science and Healing 11/1, 11-23.
Shore, A.D. (2004). Long-term effects of energetic healing on symptoms of psychological depression and self-perceived stress. Alternative Therapies 10/3, 42-48.
Singg, S. (2004). Reiki: An alternative and complementary healing therapy. In Complementary Therapies in Rehabilitation (2nd ed.), ed. by C.M. Davis, 235-52. USA: Slack Incorporated.
Sundblom, D.M., Haikonen, S., Niemi-pynttari, J., & Tigerstedt, I. (1994). Effect of spiritual healing on chronic idiopathic pain: A medical and psychological study. Clinical Journal of Pain 10/4, 269-302.
VanderVaart, S., Gijsen, V.M.G.J., de Wildt, S.N., & Koren, G. (2009). A systematic review of the therapeutic effects of Reiki. The Journal of Alternative and Complementary Medicine 15/11, 1157-69.
Vitale, A. (2007). An integrative review of Reiki touch therapy research. Holistic Nursing Practice 21/4, 167-79.
Walach, H. (2007). Spiritual and alternative cancer therapies: Strange theories, perhaps wrong, but useful. Breast Care 2, 190-92.
Winstead-Fry, P., & Kijeck, J. (1999). An integrative review and meta-analysis of therapeutic touch research. Alternative Therapies 5/6, 58-67.